Monosynaptic reflexes
- Knee reflex
- Stretch receptor in tendon –> stretch–> afferent to spinal cord –> synapse directly to efferent –> motor neuron –> contraction of extensor.
- Doesn’t have cortical input
- Fast
Polysynaptic reflexes
- Afferent and efferent neuron separated by at least one interneuron.
- Withdrawal reflex
- Pain leads to ipsilateral leg contraction and contralateral leg extension
Organisation of the spinal cord
- Midbrain, pons, medulla
- Conscious tracts – Comprised of the dorsal column-medial lemniscal pathway, and the anterolateral system.
- Dorsal column – vibration, proprioception, fine touch.
- Dorsal column–> medial leminiscus(brain stem).
- UL travel in fasciculus cuneatus.
- LL travel in fasciculus gracillis.
- Decuss in medulla as second order neuron which goes to thalamus(ventral posterolateral nucleus).
- Third order neuron: Thalamus–> internal capsule–> sensory cortex.
- Anterolateral spinothalamic tract – crude touch, pressure.
- Lateral spinothalamic tract – pain, temperature
- Both enter and ascend 1-2levels then terminate in dorsal horn(substantia gelatinosa).
- 2nd order decusses, separate into the two tracts and rises to thalamus(ventral posterolateral nucleus)
- Then third neuron–> internal capsule to sensory cortex.
- Unconscious tracts – Comprises of the spinocerebellar tracts. – balance
- Descending tracts
- Cortex –> internal capsule(between thalamus and basal ganglia)–> crus of cerebri–> midbrain/pons/medulla–> divides into lateral and anterior corticospinal tracts–> terminate in ventral horn at synapse with lower motor neuron.
- Lateral tract decuss at medulla while anterior spinal tract descends to cervical/thoracic level then decuss.
Sensory homonculus
- Sensation of various parts of the body occupies different amount of the sensory cortex reflecting the depth of sensory detail in each body part- this is the visual representation.
Visual pathways and lesions
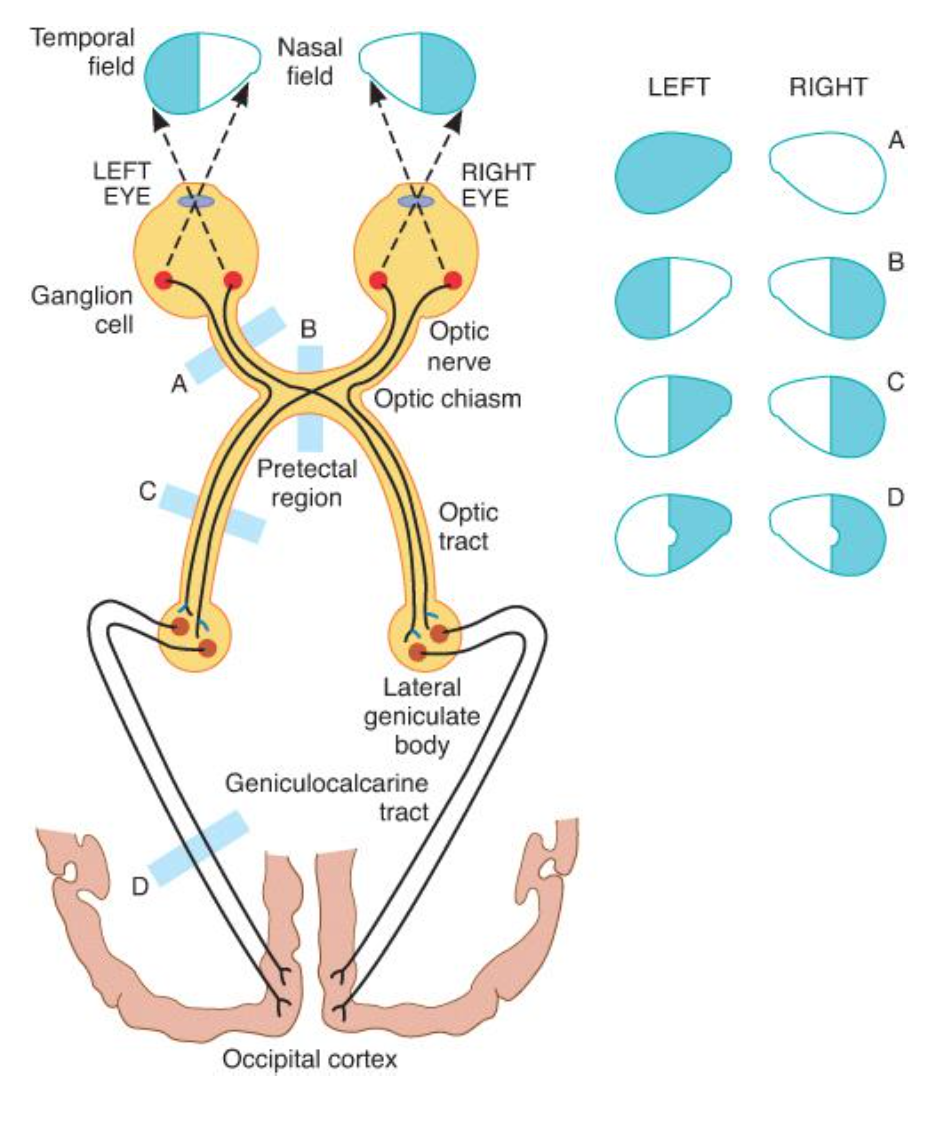
Ganong’s Review of Medical Physiology, 24th Edition
LP – lower quadrant is via Parietal radiation. Upper is Temporal radiation.
Pupillary reflexes
- Sensory – CN 2 –> CN3 leads to pupillary constriction in both eyes.
- Accomodation is also via CN3
Overview of anatomy and auditory pathways.
External ear captures sound and funnels it –> tympanic membrane vibrates–> transmitted by the stapes, incus and malleus(who act as step down with help from stapedius and tensor tympani) to oval window of inner ear –> hair cells in cochlea activate at different frequencies –> change sound energy to electrical energy and transmit to brain via CN 8.
Tuning fork tests
- Webber – place tuning fork in middle
- Normal – hear it equal on both sides
- In sensory deafness –> hear it louder in normal ear
- In conductive deafness -> increase bone conduction–> hear it in the affected ear
- Rinne – placed on mastoid process then near ear canal
- Sensory deafness – can hear it after placed near canal if partial loss
- In conductive deafness -> increase bone conduction–> cant hear it after placing next to ear canal
Vestibular function is worth a quick look too (particularly nystagmus and caloric stimulation)
Mediated by the three semi-lunar canals via CN 8
Vivas
- Tell me about the stretch reflex
- Explain the sensory and motor tracts o the spinal cord
- What is the effect of various lesions to the visual pathways
- How does the pupillary reflex work